

Prof. Ayman Hegab is a Professor of Oral & Maxillofacial Surgery, Faculty of Dental Medicine. Al-Azhar University. Cairo. Egypt.
Introduction:
Fracture of the jaw plays an important role in the practice of the oral surgeon. The mandible is the most common of the facial bones to fracture. This is due to it is relatively prominent position in relation to common injuring forces (1-4). Several authors have reported that the presence of teeth may be one of the determinants of mandibular fractures. Similarly, the incidence, treatment methods, healing rate, and post-treatment complications of these fractures also may be influenced to a greater or lesser degree by the state of dentition (5, 6).
In the words of Halozenetis, “Weak regions of the mandible have not been adequately determined. However, it has been suggested that the presence of third molar teeth may decrease the resistance of the mandibular angle region to fracture ”(7). The results of other studies confirm that patients with lower third molar present have an increased risk for angle fractures. Furthermore, it also showed that the risk for an angle fracture varied depending on lower third molar position (8-12).
Kim concluded that the mandibular angle that has a lower third molar is more susceptible to fracture when exposed to an impact than an angle without a lower third molar (13). The result of the retrospective investigation that was done by Lida et al showed that an incompletely erupted lower third molar decreases the risk of condylar fractures and increases the risk of mandibular angle fractures (14).
The aim of this study was to compare some of the clinical aspects of dentulous mandibular fractures and examine the effect of presence of lower third molars on the incidence of mandibular angle fractures.
Patients & Methods:
This study was a retrospective investigation that used patient records and radiographs as data sources. Fifty dentulous patients (43 male and 7 female, the age range was from 19-48 years with average age 24 years) with mandibular fractures treated by intermaxillary and rigid fixation at the Al-Azhar University Hospitals during the period from 2001-2006.
The medical records and panoramic radiographs, C.T and 3D C.T (figures 1-4) of 50 patients with mandibular angle fractures were examined. The presence and absence and degree of impaction of the lower third molar were assessed for each patient and related to the occurrence of fracture of the mandibular angle in addition to evaluate the degree of displacement of the fracture.
Each fracture was divided into two groups.
Group I:
Consisted of mandibular angle fractures associated with presence of lower third molar.
Group II:
Consisted of mandibular angle fractures not associated with presence of lower third molar.
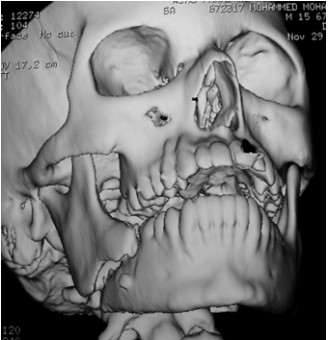
Fig 1: 3D C.T of displaced mandibular angle fracture

Fig 2: Coronal C.T of displaced angle fracture associated with impacted lower third molar
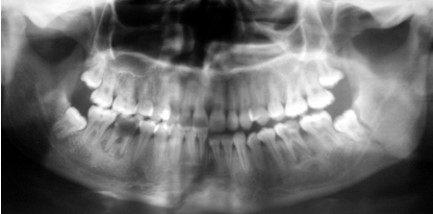
Fig 3: Panoramic radiograph of angle fracture associated with third molar.

Fig 4: Panoramic radiograph of bilateral angle fracture (sever displacement of the left , , side not associated with third molar)
Results:
The incidence of mandibular angle fracture was found to be greater when a lower third molar was present. Patients exhibiting angle fractures associated with third molar represented 74 % of all angle fractures in this investigation.
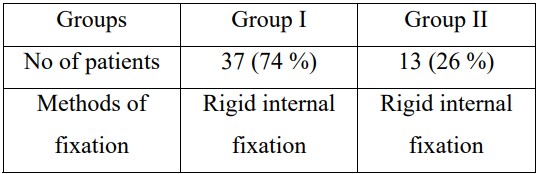
The numbers of patients and methods of fixation in both groups is shown in Table 1
Table 1: Number of patients and methods of fixation among the groups
There was a considerable difference in the sex distribution and in the causes of fractures between those with and without third molar teeth. Different causes and the distribution of sex and age are shown in Table 2.
Table 2: causes and the distribution of sex and age within the groups
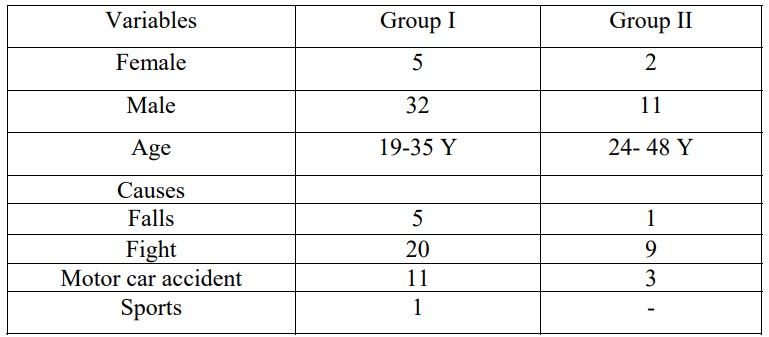
In our study, there was a considerable difference in the sex distribution and in the causes of fractures between those with and without third molar teeth, with fight representing 58% of all mandibular fracture and more with male patients.
Also, there was a difference in the age distribution between the two groups as group I was associated with younger age.
In this study, 7 cases associated with impacted third molar represented sever displacement of the angle fracture (figure 1, 2) and interfered with achievement of reduction. In four cases, extraction of the impacted lower third molar was done to achieve good reduction at the fracture site. The remaining three cases that were treated without extraction of the lower third molar required more time to obtained good reduction (time range from 30-45 minutes) and exhibited postoperative infection and delayed healing in the fracture site and underwent a second operation for removal of the lower third molar.
Only two cases without lower third molar in the fracture site represented sever displacement of the angle fracture (figure 4).
DISCUSSION:
Angle fractures were caused mainly by assault, although this is perhaps not the case for the elderly who do not frequently get involved in fights (15-16).
Wolujewicz (17) addressed the issue of buried teeth within the angle region as a predisposing factor to its weakness and concluded that there was no relationship between the state of eruption of the respective lower third molar and the incidence of angle fractures.
Oikarinen and Malmstrom (18) showed that the region of the angle was involved in more than 17% of all maxillofacial fractures in a series of 1248 cases reviewed.
Halozenetis (7) stated that angle fractures are twice as likely to occur in dentate patients compared with edentulous persons. More recently, this was confirmed by Amaratunga (5).Neither of these last two authors made specific reference to the presence or absence of third molar teeth in fractures of the angle of the mandible.
As for age ;Oikarinen and Malmstrom (18) reported a peak incidence of angle fractures in the 20 to 29 year age group. This figure is supported by data provided by Ueno et al. and Ellis et al.
Halozenetis showed that between the age of 12 to 29 years, 69% of single mandibular fractures occurred at the angle and this because that time is time for formation of the lower third molar tooth follicle and eruption of the tooth(7,8). This investigation presented clinical evidence that third molars weaken the angle of the mandible predisposing to fracture (19-21) .
In this study, mandibular angle fracture associated with lower third molar represented 74 % of all cases and this result provided an evidence that third molar tooth represents a weak point of the mandible that lowers the resistance of the bone to fracture. This result is in agreement with the result of researches of Lee et al ,Ugboko et al ,Joyce et al, Kim and Linda et al (10-14) .
In our study, the presence of completely impacted lower third molar provided more risk not only to the fracture but also to degree of the displacement of the fracture site because the tooth occupies more osseous space which could affect the postoperative result. This result agreed with the result of the study that was done by Reitzik et al (22) .
Conclusion:
The results of the present study provide data to support the commonly held view that the presence of third molar teeth provide an area of potential weakness of the mandible and predispose the angle region to fracture and exposes the fracture for many complications like postoperative infections and delayed healing. Fights accounted for the largest number of fractures .In our study; the number of fractures of the mandible caused by fights and accidents was higher in males than in females
References
1-Safdar N, Meechan JG. Relationship between fractures of the mandibular angle and the presence and state of eruption of the lower third molar. Oral Surg Oral Med Oral Pathol Oral Radiol Endod: 79:680-4,1995
2. Kruger GO. Textbook of Oral and Maxillofacial Surgery, 5th ed. St. Louis, CV Mosby. pp.397, 1979.
3. Killey HC. Fracture of the Mandible. 2nd ed. Bristol. John Wright & Sons Limited. pp. 9-25, 1971.
4. Weis L. Static loading of the mandible. Oral Surg Oral Med Oral Pathol., 19:253-62, 1965.
5. Amaratunga NA. A comparative study of the clinical aspects of edentulous and dentulous mandibular fractures. J Oral Maxillofac Surg., 48:3-5, 1988.
6. Zorman D, Godart PA, Kovacs B, Andrianne Y, Daelemans P, Burny F. Treatment of mandibular fractures by external fixation. Oral Surg Oral Med Oral Pathol., 69:15-9, 1990.
7. Halazonetis JA. The weak regions of the mandible. Br J Oral Surg., 6:37, 1968.
8. Ma?aita J, Alwrikat A. Is the mandibular third molar a risk factor for mandibular angle fracture? Oral Surg Oral Med Oral Pathol Oral Radiol Endod., 89:143-6, 2000.
9. Meechan JE, Safdar N. Lower third molars and mandibular angle fractures. Br. Dent J., 180:169, 1996.
10. Lee JT, Dodson TB. The effect of mandibular third molar presence and position on the risk of an angle fracture. J Oral Maxillofacial Surg., 58:394-8, 2000
11. Ugboko VI, Oginni FO, Owotade FJ. An investigation into the relationship between mandibular third molars and angle fractures in Nigerians. Br J Oral Maxillofacial Surg., 38:427-9, 2000.
12. Joyce T.Lee and Thomas B. Dodson: The effect of mandibular third molar presence and position on the risk of an angle fracture. Int J Oral Maxillofacial Surg.31(2): 140- 144,2002
13. Kim HK. Relationships between mandibular angle fracture and state of the lower third molar . J Korean Assoc Oral Maxillofac Surg.30(6):530-535,2004.
14.Lida S, Nomura K, Okura M and Kogo M: Influence of the incompletely erupted lower third molar on mandibular angle and condylar fractures. J Trauma. 57(3):613- 7,2004
15.Lamberg MA. Maxillofacial fractures: an epidemiological and clinical study on hospitalized patients. Proc Finn Dent Soc., 74:113, 1978.
16. Ueno T, Oka T, Miyagawa Y, Kobayashi Y. Clinical and experimental studies on the location and lines of mandibular fractures. Bull Tokyo Meed Dent Univ., 4:2 45-51, 1957.
17. Wolujewitz MA. Fractures of mandible involving the third molar tooth: an analysis of 47 cases. Br J Oral Surg., 18:125-31, 1980.
18. Oikarinen VJ, Malmstorm M. Jaw fractures:a roentgenological and statistical analysis of 1248 cases including a special study of the fracture lines in the mandible drawn from ortopanthomograms in 660 cases. Suom Hammaslaak Seur Toim., 65:95- 111, 1969.
19. Ellis E, Moos KF, El-Attar A. Ten years of mandibular fractures:an analysis of 2137 cases. Oral Surg Oral Med Oral Pathol., 59:120-9, 1985.
20. Meechan JE, Safdar N. Lower third molars and mandibular angle fractures. Br. Dent J., 180:169, 1996.
21. Lee JT, Dodson TB. The effect of mandibular third molar presence and position on the risk of an angle fracture. J Oral Maxillofacial Surg., 58:394-8, 2000.
22. Reitzik M, Lownie JF, Cleaton-Jones P, Austin J. Experimental fractures of monkey mandibles. Int J Oral Surg 1978;7:100-103.
