


Prof. Ayman Hegab is a Professor of Oral & Maxillofacial Surgery, Faculty of Dental Medicine. Al-Azhar University. Cairo. Egypt.
Introduction:
Since the first description of a surgical reduction of a zygoma fracture by Duverney (1) in 1751, many varying methods of treatment have been described. Both intraoral and extraoral methods have become commonplace. The transoral approach was popularized by Keen (2) in 1909, with later modification by Goldthwaite (3) and Quinn (4). These techniques offer the advantages of avoiding any skin incision, thereby avoiding any visible scaring. Additionally, they allow for minimal dissection and excellent vector for reduction; however, they may result of increased rate of infection by introducing oral flora into the infratemporal fossa. Gilles et al (5) described the temporal fossa approach in 1927, and this becomes a very popular method for treatment of isolated arch fractures around the world. Similarly, Dingman and Natvig (6)described the supraorbital approach as an extraoral alternative in 1964. All of these techniques have in common the use of a Rowe zygoma elevator, Kelly hemostat or similar instrument placed between the arch and coronoid process to achieve reduction. Others have described several percutaneous methods meant to be less invasive, these include passing wire beneath the arch or using a towel clip to directly grasp the bone fragments and allow for lateral force to be applied. The use of a towel clip passed beneath the arch has been described previously in a case series by Hwang and Lee (7), but little description of the procedure was offered. Todd et al (8) in 2005 used a large towel clip for reduction of the depressed zygomatic arch fracture by opening the towel clip widely and one tine is introduced and passed deep to the depressed arch and then the towel clip is partially closed and the inferior tine of the towel clip is then passed and the clip is closed and firm, steady lateral force is applied to reducing the arch into appropriate position In 2002, Jochen et al(9) reported a modified surgical technique for treatment of isolated arch fracture. This technique describes an endoscopic approach which allows mere elevation and osteosynthesis of arch fracture.
Patients &Methods:
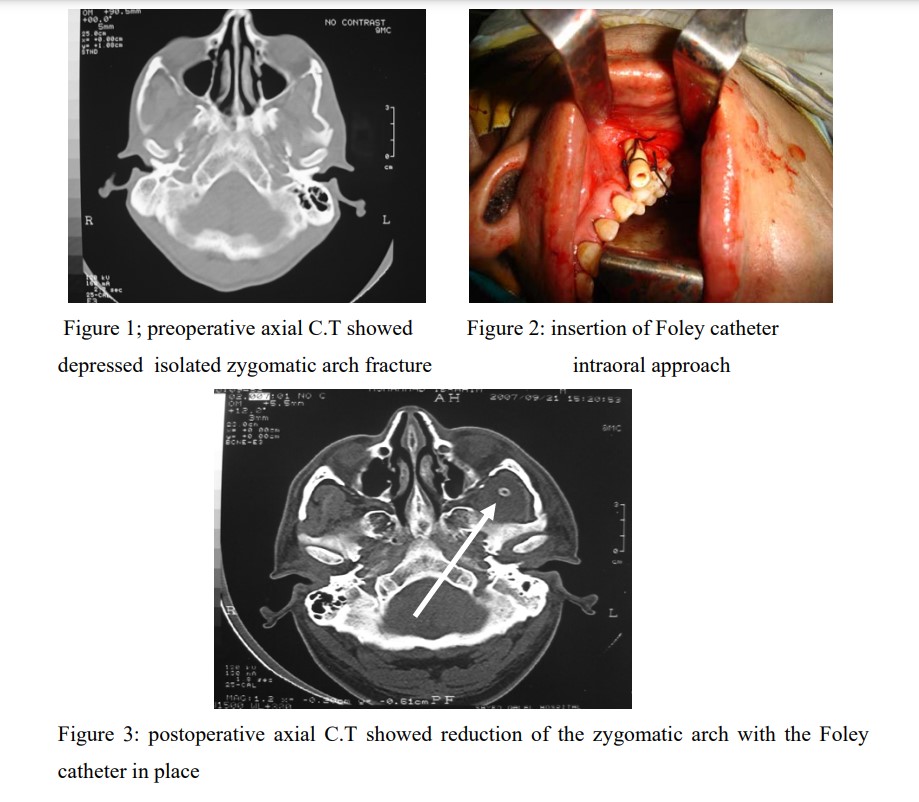
Five patients with isolated depressed Zygomatic arch fracture were included in this study. The type and the extent of the fracture were diagnosed by computed tomographic scan in axial plane (figure 1). Intraoral approach (keen approach) was used for reduction of the Zygomatic arch using the Rowe zygoma elevator and insertion of the Foley Catheter under the Zygomatic arch (figure 2). Normal saline was used to inflate the Foley Catheter balloon for stabilization of the Zygomatic arch. In one patient, the displacement of the arch was mild and in such case, the Foley catheter was used for reduction and stabilization of the displaced arch. Immediate postoperative axial C.T was used for evaluation of the reduction of the Zygomatic arch and for evaluation of the position of the Foley catheter (figure 3). The Foley catheter was removed after three weeks.
Results:
Stabilization of the Zygomatic arch fracture by the Foley Catheter was done and the fracture alignment was established perfectly. One patients’ exhibits infection at the intraoral approach treated with antibiotic for five days and two patients reveal difficulty in mouth opening with the catheter balloon in place and this compliant disappeared after removal of the catheter. One year follow-up showed good functional and cosmetic results. None of the patients showed evidence of disturbance of the facial nerve function or persistent trismus.
DISCUSSION:
Foley catheter has been used in maxillofacial fracture management previously. Edgerton and Williams (10) stabilized the orbital floor fractures with a Foley catheter inflated in the maxillary sinus. Gatot and Towi (11) also presented pediatric cases treated with the same method. Foley catheter inserted via Gillies approach can be an alternative for the stabilization of unstable isolated Zygomatic arch fracture. Placement of the catheter is very easy and safe because of the anatomical space present under the deep temporal fascial. After the reduction of the zygomatic arch fracture there is an empty place that can be filled with the balloon of the catheter. The position of the catheter can be changed easily if necessary after CT control. The potential disadvantages of the method are infection, pressure injury of the adjacent tissues and dead space after removal of the catheter. Unstable zygomatic arch fracture can be stabilized either by internal fixation, external traction or internal supporting.Internal fixation necessitates an open reduction which is a major procedure. External traction with a transcutaneous K-wire as described by Rohrich et al.(12) has two drawbacks: first, the wire pulls the arch from a single point which is not the optimum stabilization and second, there is a risk of nerve damage of the frontal branch. The successful result obtained in our study suggests that this method may be a logical, simple, easy and useful approach in the treatment of unstable isolated zygomatic arch fractures.
Conclusion:
Stabilization of the Zygomatic arch using the Foley catheter balloon through the intra oral approach is a simple procedure provided adequate stabilization to the fractured arch without extraoral scar. Reduction of the Zygomatic arch using this technique can be done only in recent, mild displaced Zygomatic arch fracture.
References
1- Duverney JG: La fracture de l, apophyse zygomatique.Traite des Masladies Os.1:182,1751 .
2- Keen WW: Surgery: its principles and practice. Philadelphia, PA,Saunders,1909 .
3- Goldthwaite RH: Plastic repair of depressed fracture of lower orbital rim.JAMA.82:628.1924 .
4- Quinn JH: Lateral coronoid approach for intraoral reduction of fractures of the Zygomatic arch. J Oral Surg, 35: 321, 1977 .
5- Gilles HD, Kilner TP, Sone D: Fractures of the malar-zygoma compound, with a description of a new x-ray position. Br J Surg, 14: 651,1927 .
6- Dingman RO and Natvig P: Surgery of facial fractures. Philadelphia, PA,Saunders, pp 211-245. 1964 .
7- Hwang K and Lee SI: Reduction of Zygomatic arch fracture using a towel clip. J Craniofac Surg. 10: 5, 1999.
8- Todd G, Carter, Sbabrokb Bagberi and Eric J, Dierks:Towel clip reduction of the depressed zygomatic arch fracture.J Oral Maxillofac Surg: 63:1244, 2005.
9- Jochen A, Werner, Jan-Eric Frenkler, Burkard M, Lippert and Benedikt J, Folz: Isolated zygomatic arch fracture: Report on a modified surgical technique. Plastic and Reconstructive Surgery.109(3): 1085,2002 .
10- Edgerton MT, Williams GS. The mouth, tongue, jaws and salivary glands. In: Sabiston Textbook of Surgery, The biological basis of modern surgical practice, 10th Ed. WB. Philadelphia, Saunders Company, 1233-74. 1972 .
11- Gatot A, Tovi F. Early treatment of orbital floor fractures with catheter balloon in children. Int J Ped Otorhinolaryngol; 21: 97-102. 1991 .
12- Rohrich RJ, Hollier LH, Watumull D. Optimizing the management of orbitozygomatic fractures. Clin Plast Surg; 19: 149. 1992 .
