

Ranula
A ranula (Latin word rana, meaning frog) describes a blue, translucent swelling in the floor of the mouth, reminiscent of the underbelly of a frog.
It is an uncommon type of mucus-filled cyst (mucocœle arising from the sublingual or submandibular salivary glands in the floor of the mouth ) .

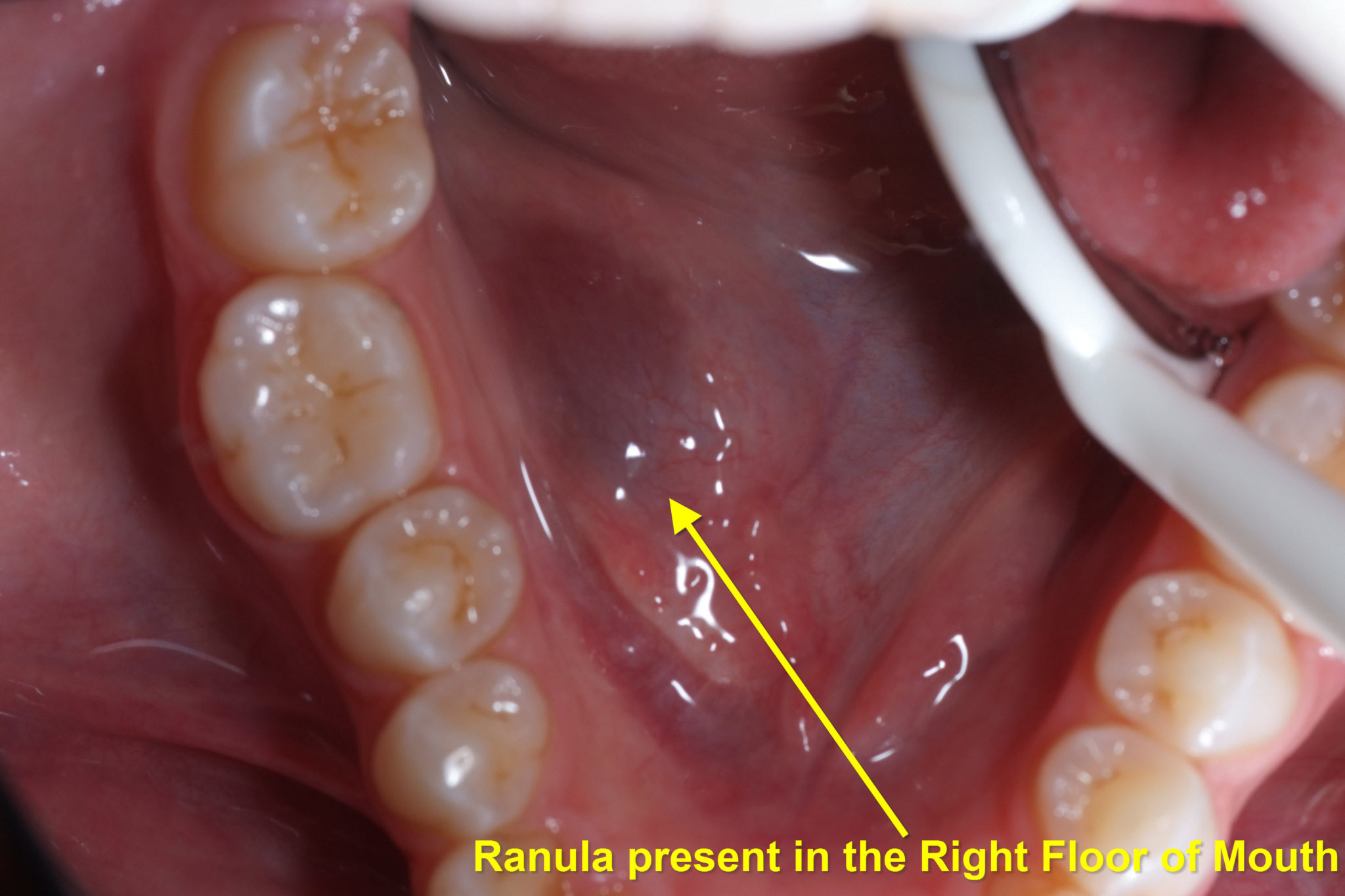
Photo showing Gustatory Sweating (arrowed). The Superficial Parotidectomy scar can be seen.
The structure is essentially the same as other mucocœles , though there is usually an epithelial lining (i.e. lined by “skin”).
Ranulae are usually either one-side or the other in the floor of the mouth and 2 – 3 cm in diameter. Occasionally, they extend across the whole of the floor of the mouth.
A ranula is most commonly observed as a bluish cyst located below the tongue. It may fill the mouth and raise the tongue. Typically, these are painless masses that do not change in size in response to chewing, eating or swallowing but may interfere with these functions (speech or chewing / eating). Occasionally, pain may be involved.
Ranulae are rare. In one study of 1303 salivary gland cysts, only 42 were ranula . The reported male-to-female ratio of occurrence is 1:1.3. Ranula tends to occur most frequently in the second and third decades of life, with an age range of 3 – 61 years.
Ranula Formation
Ranula are formed from 1 of 2 processes:
1- Partial obstruction of a sublingual duct can lead to formation of an epithelial-lined retention cyst. This is unusual, occurring in less than 10% of all ranula
2- Trauma can lead to formation of ranula. With trauma, if a duct is obstructed, secretory back-pressure builds leading to salivary duct rupture with mucus being forced into the surrounding tissues. Alternately, trauma causes direct damage to the duct or acini, leading to mucus extravasation a pseudocyst then forms. The more appropriate term for this may be Mucus Escape Reaction (MER).
Ranula Investigations
MRI is the most sensitive imaging study to evaluate the sublingual gland and its pathologic states.
Sublingual glands and their pathologic states are difficult to visualise with ultra-sound.
Obtaining a specimen for pathology is essential, not only for histologic confirmation but also because the presence of squamous cell carcinoma arising in the cyst wall of a ranula and papillary cystadenocarcinoma of the sublingual gland presenting as a ranula have been reported.
Medical Treatment
A recent though small study evaluated the effectiveness of orally administered Nickel Gluconate-Mercurius Heel-Potentised Swine Organ Preparations D10/D30/D200, a homo-toxicological agent.
This medication acts to stimulate pseudocyst re-absorption and glandular repair and aids in improving the physiologic functioning of the gland. In this study, Nickel Gluconate-Mercurius Heel-Potentised Swine Organ Preparations D10/D30/D200 was administered regularly from 6 weeks to 6 months. Eight out of 9 ranula responded to medical therapy.
Surgical Treatment
Marsupialisation: Simple marsupialisation is the oldest and most widely reported treatment for ranula. It involves ‘unroofing’ the cyst and tacking the edges of the cyst to adjacent tissue.
Failure rates range from 61 – 89% with cysts recurring anywhere from 6 weeks to 12 months later.
Inferior compression on the cyst from the tongue leads to premature closure of the opened cyst leading to the high recurrence rates. When conventional marsupialisation is undertaken, the wound margins tend to be in contact with each other because of the narrow space and the movement of the tongue and the floor of the mouth. As a result, the ranula tends to re-form and recur. Packing the cyst cavity with gauze for 7 – 10 days improves the success rate.
Placement of suture / stitch or Seton: A silk suture or Seton can be placed through the surface of the cyst under local anaesthesia. This is left in place while an epithelial tract forms, to allow for mucus drainage between the surface and the underlying salivary glandular tissue.
Morbidity is minimal to non-existent and success has been good in limited studies.
Sclerosing Agents: Bleomycin and OK-432 have been used with success in treatment of ranul?.
In one study, 31/32 patients (97%) achieved a disappearance or marked reduction in ranula size with injection of OK-432. Nearly half of all patients experienced local pain or fever which resolved over several days. Intra-cystic injection therapy with OK-432 is relatively safe and can be used as a substitute for surgery in the treatment of ranul?. Intra-cystic sclerosing injection with OK-432 has been proposed as a ranula primary treatment.
CO2 Laser: The CO2 laser has been used with a limited number of patients with good success to remove the cyst and scar the gland enough to decrease risk for recurrence.
Post-operative follow-up at 6 months showed no recurrence, no lingual nerve dysaesthesia , no ductal disruption and only minimal scar formation.
Radiation Therapy: In the rare patient who cannot tolerate surgery, radiation therapy is a viable alternative. Low doses are effective. Xerostomia (dry mouth) can be avoided with low-dose therapy and shielding of the opposite side parotid gland. The risk of radiation-induced malignancy is real but small.
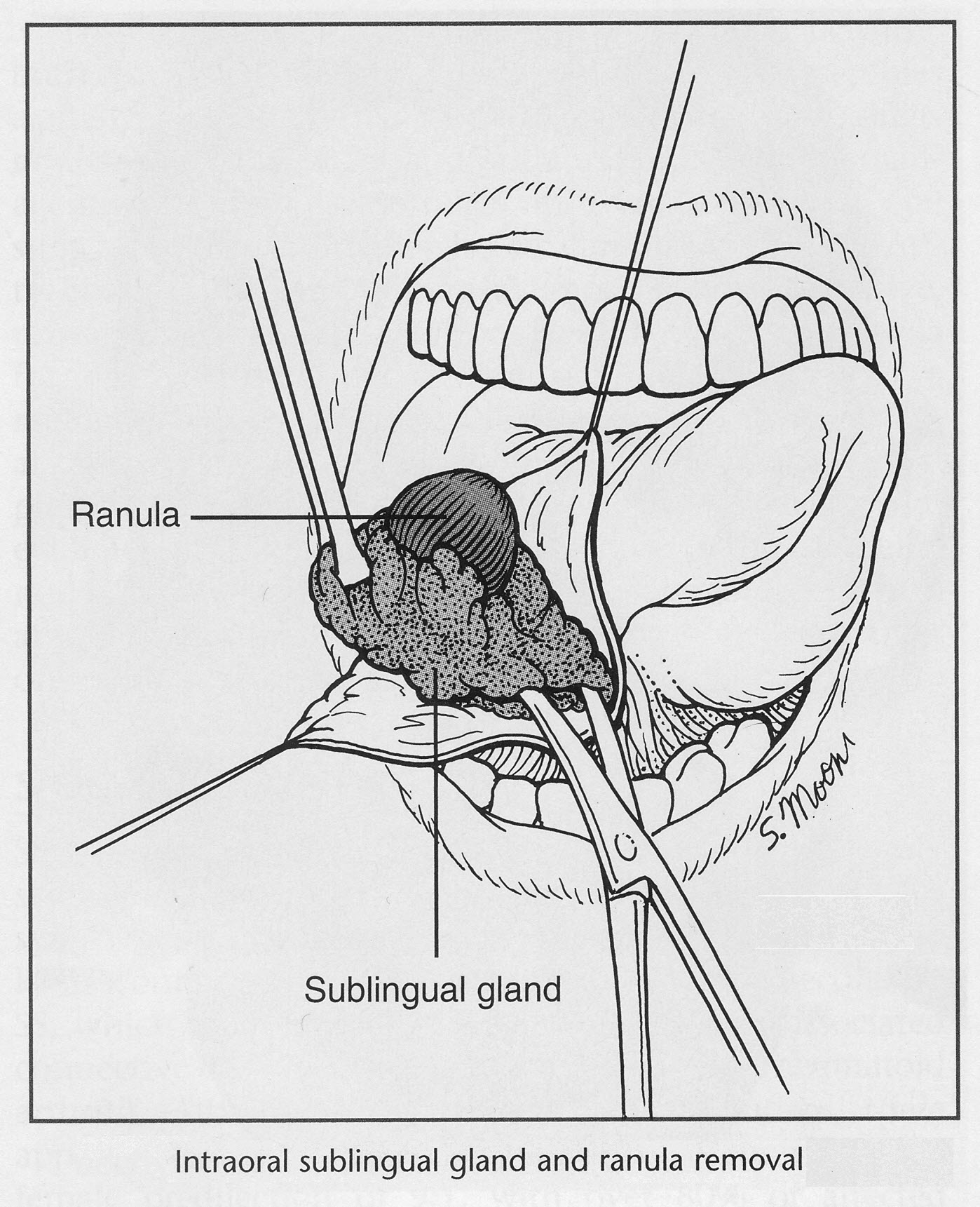
Sublingual Gland Excision: The ‘gold-standard’ treatment for ranula; is the excision of the ranula & the sublingual gland . This removes the source of the mucus and thus significantly decreases the risk for recurrence.
A ranula larger than 1 cm should be treated by removal of the offending sublingual gland; other authors have proposed that this treatment be used regardless of the size of the lesion. Marsupialisation, excision of the ranula alone and excision of the sublingual gland combined with the ranula resulted in recurrence rates of 66.67%, 57.69% and 1.20% respectively.
Some authors advocate the injection of methylene blue into the ranula at the start of the procedure to improve the preservation of vital surrounding structures. Care must be taken as the dye can leak into (non-ranula) surrounding tissue and be misleading to the surgeon.
Complications
Ranula surgical treatment involves the following risks:
- recurrence of the ranula (especially when the sublingual gland was not removed).
- damage to the lingual nerve resulting in paraesthesia (numbness) of the nerve (up to 25% in some studies). The tongue numbness generally resolves over the course of six months.
- injury to the Wharton duct with the possibility of obstructive sialadenitis and ductal laceration leading to salivary leakage.
- severe haemorrhage from the lingual and sublingual vasculature
- post-operative haematoma
Baurmash recommended that ranula be treated initially by marsupialisation with packing and, if recurrence occurs, the offending sublingual gland should then be excised.
The essential treatment of a ranula was meticulous dissection of the thin wall of the cyst in continuity with the Sublingual Gland of origin . Fibrin glue was injected into the cystic space of the ranula after it had been evacuated by aspiration. The fibrin glue within the cystic cavity prevents collapse of the wall of the cyst during surgery and facilitates and simplifies the surgical procedure by clearly outlining the involved area and by sharply delineating its thin wall.
Outcome and Prognosis
The overall risk for recurrence when the sublingual gland is not excised has been reported to be in excess of 50%.
This rate drops to as low as 2% if the gland is excised. As the risk to adjacent structures is higher for gland-excising procedures, a trial of less-invasive procedures is advocated by some.
Smaller cysts (< 1.5 cm) are usually more superficial in nature and may respond more readily to marsupialisation. Larger cysts are more closely associated with the gland and usually require gland excision in association with cyst removal.
