

The objective of exposing ± bonding a bracket on to an unerupted tooth is to move the tooth into a good functional & aesthetic position.
Exposure of a tooth at its simplest, consists of removing the gum overlying the crown of the unerupted tooth under Local An?sthetic. Most unerupted teeth are deeper within the jaw and require the removal of bone as well as the gum to expose and disimpact them; as a consequence, this may be done under General An?sthetic.
The application of traction (using the chains attached to braces) to stimulate and guide the eruption of buried teeth is necessary as the teeth are unfavourably angled (and spontaneous eruption is inhibited), where buried teeth are obstructed from eruption by other teeth & where teeth are exposed long after their root development is complete.
Teeth most likely to be exposed and bonded are the upper canines / eye teeth, upper central incisors, molars and the occasional premolars.



The medico-legal landscape of consent has been shaped by a number of cases, such as Chester v Afshar [2004], Montgomery v Lanarkshire Health Board [2015], Duce v Worcestershire Acute Hospitals NHS Trust [2018] amongst others, so that it is more patient-centred.
Many of the legal claims in surgical (& medical) cases occur as a result of “failure to warn”, i.e. lack of adequately documented and appropriate consent.
A pre-requisite for obtaining consent for a surgical (medical / dental) procedure from a patient, is a full exchange of information regarding any risks, drawbacks and limitations of the proposed treatment and any alternatives to it (even non-treatment).
The clinicians should provide the patient with as much information as is appropriate and relevant, that it should be in terms the patient understands & the risks should be personalised for that individual patient. Also, there should be enough time for the patient to understand the information given and get a second opinion if needs be.
This list of warnings might seem excessive to some however the legal ruling in the case of Chester vs Afshar (2004) would suggest that it is quite prudent / necessary to list them. Others might say that there isn’t enough information but where do you stop?

The following list of warnings regarding tooth exposure & bonding is neither exhaustive nor is it predictive. The most pertinent warnings have been included here.
You are to have a tooth exposed ± bracketed. You can expect the following:
The extraction site will often be closed with stitches. These are dissolvable and ‘fall out’ within 10 – 14 days. If a pack has been sewn in or the chain is ‘parked’ high up in the sulcus, non-dissolving stitches are used, that will need to be removed at some point.
Exposing ± Bracketing of Tooth Specific Warnings:
Stitches.
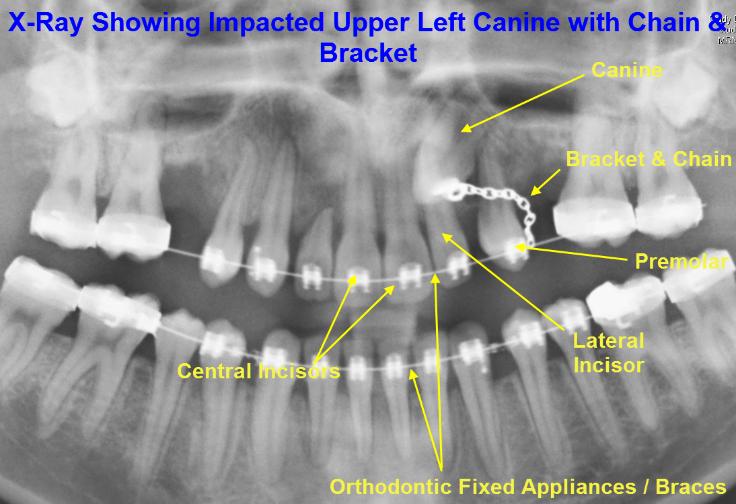
Brackets.
These are small golden plaques with chains attached. These are stuck onto the teeth that need to be moved. Sometimes, the cement sticking the chain onto the tooth can break after traction is applied to the tooth; if this happens, the bracket will need to be re-cemented on. Occasionally, the chain itself breaks and this will mean that the chain and bracket have to be replaced.
Gauze Pack.
Sometimes, it is not possible to stick the chains onto the teeth. If this is the case, a gauze pack impregnated with an antiseptic (BIPP) is placed over the exposed tooth and sewn into place. The pack is removed after approximately a week and the chain will be stuck on at this point.
Ankylosis of Tooth.
Occasionally, even if the tooth has traction applied to it, it still refuses to move. If this happens, it is sometimes necessary to explore the area – there may be a lip of bone preventing the tooth from moving or the tooth has fused with the surrounding bone (ankylosis).
Repeated Operation.
The gum can easily grow back over the exposed tooth. If this is the case and the tooth doesn’t have a bracket stuck on it, the tooth will need to be re-exposed, hence another operation.
General Surgical Warnings:
Pain.
As it is a surgical procedure, there will be soreness after the procedure. This can last for several days. Painkillers such as ibuprofen, paracetamol, Solpadeine or Nurofen Plus are very effective. Obviously, the painkiller you use is dependent on your medical history & the ease with which the tooth was exposed.
Swelling.
There will be swelling afterwards. This can last up to a week. Use of an icepack or a bag of frozen peas pressed against the cheek adjacent to the tooth removed will help to decrease the swelling. Avoidance in the first few hours post-op, of alcohol, exercise or hot foods / drinks will decrease the degree of swelling that may develop.
Bruising.
Some people are prone to bruise. The bruising can look quite florid; this will resolve but can take several weeks (in the worst cases).
Limited Mouth Opening.
Often, the chewing muscles and the jaw joints are sore after the procedure so that mouth opening can be limited for the next few days.
