

Upper Jaw Fraenum.
A ‘high’ or prominent upper fraenum in children, although a common finding, is often a concern, especially when associated with a diastema (a space between 2 teeth such as the upper central incisors). Treatment is necessary only when the fr?num exerts a traumatic force on the gum or it causes a diastema to remain open after eruption of the permanent canines / ’eye’ teeth.
In an older child, if a fraenum is present and the tissue immediately behind the central incisors on the roof of the mouth side of the teeth blanches when the upper lip is pulled, removal of the fr?num is indicated.
Early treatment is also indicated to prevent subsequent inflammation, recession of the gum around the spaced teeth, pocket Tongue Tie / Ankyloglossia.
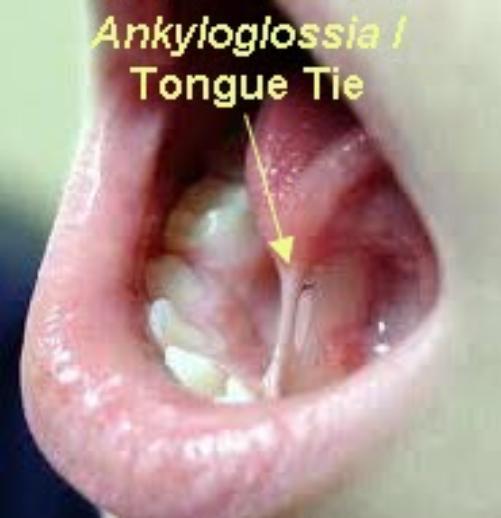
A Tongue Tie / Ankyloglossia is characterised by a short, thick fibrous band linking the tongue to the gum just behind the lower central incisors. It limits the movement of the tongue.


The significance and management of ankyloglossia is controversial. Studies have shown a difference in treatment recommendations between Speech Therapists, P?diatricians, Ear, Nose & Throat Surgeons and Oral & Maxillofacial Surgeons. Most professionals, however, will agree that there are certain indications for fr?nectomy.
A tongue tie can limit tongue movement and create swallowing problems. A fraenectomy for functional problems should be considered on an individual basis.
A tongue tie can lead to problems with breastfeeding, speech, how teeth bite together and potential gum disease and gum recession problems. The fraenectomy will only be done if evaluation shows that function will be improved by surgery.
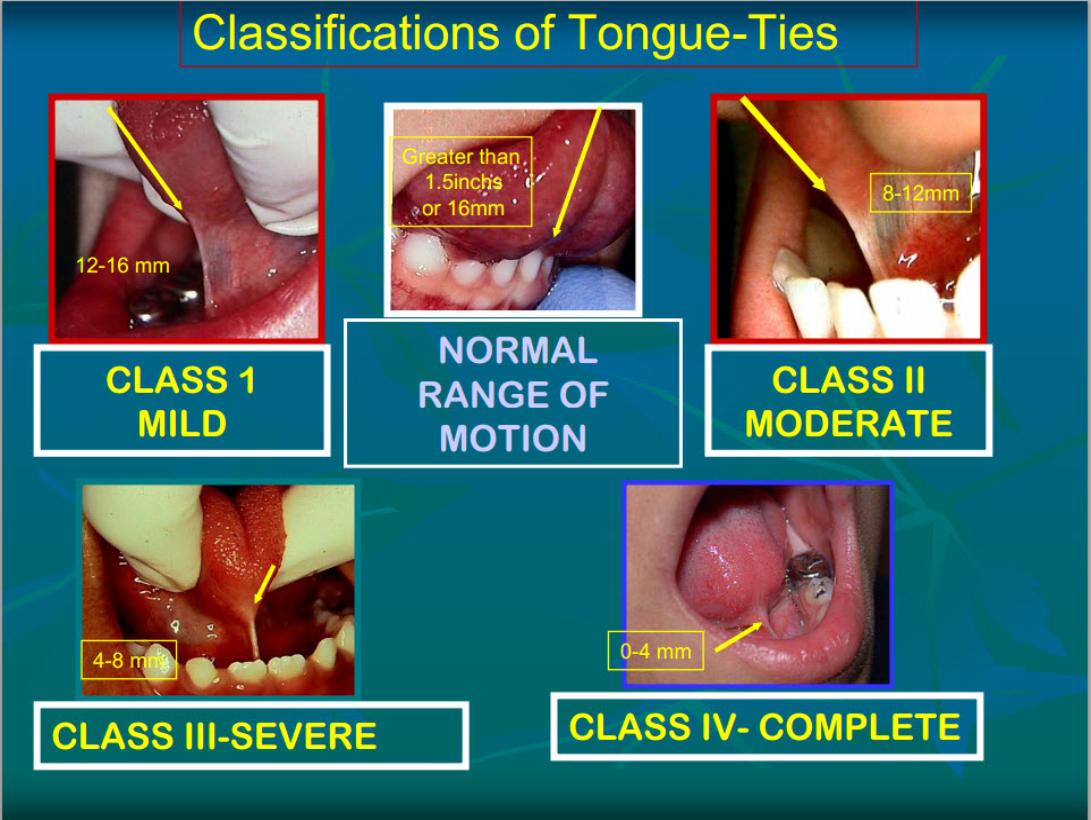
Ankyloglossia can be classified into 4 classes based on Kotlow’s Classification as follows:
- Class I: Mild ankyloglossia (12 – 16 mm)
- Class II: Moderate ankyloglossia (8 – 12 mm)
- Class III: Severe ankyloglossia (3 – 8 mm)
- Class IV: Complete ankyloglossia (< 4 mm)
Class III and IV tongue-tie categories should be given special consideration because they severely restrict the tongue’s movement.
A normal range of motion of the tongue is indicated by the following criteria:
- A positive ‘blanch test’ of the incisal papilla when pulling the lip forwards
- large midline maxillary suture present radiographically
- To facilitate orthodontic treatment for closure of a diastema
- To enhance the chances of the diastema remaining closed after orthodontic treatment
- A persistent midline diastema
- To eliminate undesirable tension on the gingival papilla or gingival margin
- To facilitate lip lengthening procedure
- To allow effective toothbrushing in the area of the fraenum
- The medico-legal landscape of consent has been shaped by a number of cases, such as Chester v Afshar [2004], Montgomery v Lanarkshire Health Board [2015], Duce v Worcestershire Acute Hospitals NHS Trust [2018] amongst others, so that it is more patient-centred.
Many of the legal claims in surgical (& medical) cases occur as a result of “failure to warn”, i.e. lack of adequately documented and appropriate consent.
A pre-requisite for obtaining consent for a surgical (medical / dental) procedure from a patient, is a full exchange of information regarding any risks, drawbacks and limitations of the proposed treatment and any alternatives to it (even non- treatment).
The clinicians should provide the patient with as much information as is appropriate and relevant, that it should be in terms the patient understands & the risks should be personalised for that individual patient. Also, there should be enough time for the patient to understand the information given and get a second opinion if needs be.
The following list of warnings regarding fraenectomies is neither exhaustive nor is it predictive. The most pertinent warnings have been included here.
Fraenectomy / Tongue-Tie Release Explanation & Warnings
A fraenum is a band of fibrous tissue that links the lips to the gums or the tongue to the gums.
Upper Jaw Fraenum.
A ‘high’ or prominent upper fr?num in children, although a common finding, is often a concern, especially when associated with a diastema (a space between 2 teeth such as the upper central incisors). Treatment is necessary only when the fr?num exerts a traumatic force on the gum or it causes a diastema to remain open after eruption of the permanent canines / ’eye’ teeth.
In an older child, if a fr?num is present and the tissue immediately behind the central incisors on the roof of the mouth side of the teeth blanches when the upper lip is pulled, removal of the fraenum is indicated.
Pain.
As it is a surgical procedure, there will be soreness after the fraenum has been removed. This can last for several days. Painkillers such as Ibuprofen or Paracetamol are very effective. Obviously, the painkiller you use is dependent on your medical history & the ease with which the fr?nectomy was carried out.
Swelling.
There will be swelling afterwards. This can last several days. Avoidance in the first few hours post-op of exercise or hot foods / drinks will decrease the degree of swelling that can develop.
Stitches.
The fraenectomy site will be closed with stitches. These are dissolvable and ‘fall out’ within 10 – 14 days.
Limited Mouth Opening.
Often the chewing muscles and the jaw joints are sore after the procedure so that mouth opening can be limited for the next few days.
Conscious Use of Tongue.
Don’t automatically assume that once the tongue tie has been released, you’ll be automatically able to stick your tongue out. You will have been used to the tongue being limited in its movements for a number of years so to fully use the ‘released’ tongue, a conscious effort will have to be made to use it.
Floor of the Mouth Complications.
This may have an effect on the salivary ducts in the region of the floor of the mouth in that the stitches may restrict the outward flow of saliva and this can lead to ballooning up of the floor of the mouth. If this is the case, get back in contact with the OMFS department / Oral Surgeon post-haste.
Repetition of Fraenectomy.
Sometimes, the degree of tongue movement is not as great as expected and may mean that the fraenectomy needs to be done again. Post-op tongue-tie release exercises are advocated by some people.
Closure of Spaced Teeth.
Having an upper fraenectomy will not necessarily by itself, produce the closure of the space. It is often an adjunct to the Orthodontic closing of the space.
Exposed, Raw Areas.
If the upper fraenum has been removed, there may be initially, an area in the midline where the gums can not be approximated; this produces a raw area that can take awhile to heal.
Gum Recession.
When the upper fraenum is removed, it is possible that the gums around the upper central incisors may recede.
Level of ‘Lip Line’.
Once the fraenum has been removed, the upper lip is freed and can ‘ride up’ higher displaying more teeth and gums (that is, showing a higher lip line).
Useful Articles & Websites
1- J Clin Diag Res 2012. Frenectomy. A Review with the Reports of Surgical Techniques
3- Wikipedia
