

The medico-legal landscape of consent has been shaped by a number of cases, such as Chester v Afshar [2004], Montgomery v Lanarkshire Health Board [2015], Duce v Worcestershire Acute Hospitals NHS Trust [2018] amongst others, so that it is more patient-centred.
Many of the legal claims in surgical (& medical) cases occur as a result of “failure to warn”, i.e. lack of adequately documented and appropriate consent.
A pre-requisite for obtaining consent for a surgical (medical / dental) procedure from a patient, is a full exchange of information regarding any risks, drawbacks and limitations of the proposed treatment and any alternatives to it (even non-treatment).
The clinicians should provide the patient with as much information as is appropriate and relevant, that it should be in terms the patient understands & the risks should be personalised for that individual patient. Also, there should be enough time for the patient to understand the information given and get a second opinion if needs be.
A pre-requisite for obtaining consent for a surgical (medical / dental) procedure from a patient, is a full exchange of information regarding any risks, drawbacks and limitations of the proposed treatment and any alternatives to it (even non-treatment).
The clinicians should provide the patient with as much information as is appropriate and relevant, that it should be in terms the patient understands & the risks should be personalised for that individual patient. Also, there should be enough time for the patient to understand the information given and get a second opinion if needs be.
Pain.
As it is a surgical procedure, there will be soreness after the biopsy. This can last for several days. Painkillers such as ibuprofen, paracetamol, Solpadeine or Nurofen Plus are very effective. Obviously, the analgesic you use is dependent on your medical history & the pain you are experiencing.
Stitches.
The biopsy will often be closed with stitches. These are dissolvable and ‘fall out’ within 10 – 14 days.
Scarring / Lumpiness at the Biopsy Site.
Any cut to soft tissues produces a scar. Initially, after a biopsy, a scar will be produced. This softens and disappears (i.e. improves) with time. Regardless, it can feel quite obvious and lumpy (especially if the biopsy has been in the lips or cheeks.
The scarring can also dependent on the size and size of the biopsy and the individuals’ tendency to scarring.
Recurrence.
Dependent on what is biopsied, there is a chance that the lesion can recur. They recur either due to the nature of the lump / patch or due to the recurrence of conditions that caused the lump / patch to develop.
For instance, during pregnancy many odd lumps and bumps develop on the gums. If they are removed / biopsied, they recur. They are often left until after the end of pregnancy as most of the lesions disappear or dramatically regress. Polyps on the cheeks or lips can recur as the patient may bite on these areas again producing the polyps anew.
Further Treatment Dependent on Results.
Depending on what the biopsy results are, will determine whether further treatment is required. If the lump turns out to be just a polyp or granuloma, then nothing further needs to be done.
If the patch turns out to be symptomatic lichen planus then steroids can be prescribed and the patch can be reviewed in initially by the hospital and then by the GDP / GMP. If the lump turns out to be more serious, then further investigations and treatments may be necessitated.
Swelling.
There will be swelling afterwards. This can last several days. Use of an ice-pack or a bag of frozen peas pressed against the cheek adjacent to the biopsy site, will help to decrease the swelling. Avoidance in the first few hours post-op, of alcohol, exercise or hot foods / drinks will decrease the degree of swelling that will develop.
Occasionally, there is bleeding into the cheek or the floor of the mouth (dependent on where the biopsy took place) – there may well be limitations to mouth opening or tongue use respectively. This also improves with time.
Limited Mouth Opening (Trismus).
Limited Mouth Opening (Trismus). Often the chewing muscles and the jaw joints are sore after the procedure so that mouth opening can be limited for the next few days.
Initial Tautness / Tenderness at the Biopsy Site.
The biopsy margins are brought together with stitches hence there is some tension at the operation site. This tails off as the swelling goes down.
Localised Area of Numbness at the Biopsy Site.
This especially effects the lips and tongue (tip). Biopsies can damage the local nerves resulting in areas of numbness. These can take a number of months before normal feeling returns.
Inconclusive Results & the Need for Re-Biopsy.
The biopsy results can come back as inconclusive. If this is the case, then it is possible that the lesion may need to be biopsied again. If all the lump / bump has been removed, it is very unlikely that these come back as inconclusive (and also there is no possibility of re-biopsying the site).
Anatomical-Specific Warnings:
Tongue – limitation mobility / function of tongue (due to swelling, tenderness etc); marked swelling.
Gums – gum recession, hot-cold sensitivity due to exposed dentine as the gum recedes; need for use of Coe-Pak (surgical dressing / cement) dressing
Cheeks – numbness / tingling at the biopsy site (especially if biopsy of lip); problems with salivary gland ducts (adjacent to the upper 1st molars) being traumatised, tied off (by stitches) or cut through.
Floor of Mouth – altered sensation; problems with salivary gland ducts being traumatised, tied off (by stitches) or cut through.
Roof of Mouth – bleeding from biopsy site due to difficulty in apposing the wound sides; roof of mouth-floor of nose communications (especially if the soft palate is being operated on); need for use of Coe-Pak.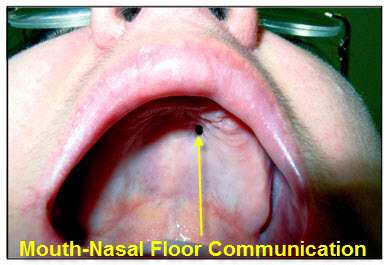
Tongue – limitation mobility / function of tongue (due to swelling, tenderness etc); marked swelling.
Gums – gum recession, hot-cold sensitivity due to exposed dentine as the gum recedes; need for use of Coe-Pak (surgical dressing / cement) dressing
Cheeks – numbness / tingling at the biopsy site (especially if biopsy of lip); problems with salivary gland ducts (adjacent to the upper 1st molars) being traumatised, tied off (by stitches) or cut through.
Floor of Mouth – altered sensation; problems with salivary gland ducts being traumatised, tied off (by stitches) or cut through.
Roof of Mouth – bleeding from biopsy site due to difficulty in apposing the wound sides; roof of mouth-floor of nose communications (especially if the soft palate is being operated on); need for use of Coe-Pak.
